by Archivist Patricia Dark
Since the passage of the Health and Social Care Act 2012, public health has been a core function of local councils like Southwark. As Professor Kevin Fenton, Southwark’s Director of Health and Wellbeing, told the Spring 2017 edition of Southwark Life, this means that “…local councils have had responsibility for helping to improve the health and wellbeing of local people… not only through commissioning health services but also taking every opportunity to promote health through work with schools, housing, transport and many other areas.”
The basic idea behind this approach is to make sure that public health efforts reflect a local area’s specific concerns and priorities. A “one size fits all” solution doesn’t work for health – different communities have different levels of education, different cultural backgrounds, and even different patterns of disease. Public health awareness needs to be tailored to local cultural expectations, focus on the issues that are most likely to be harmful, and provided in language that everyone can understand. Very often, local authorities are best placed to adapt to local conditions, tailor messages to local cultures, and to serve local needs.
Two realisations underpin this shift toward joined-up, locally-based public health: first, that it’s simply cheaper and easier to keep people healthy than it is to make them healthy once they are sick, and second, health is more than not being sick. The preamble to the constitution of the World Health Organisation, which was ratified in 1946, defines health as “…a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.” Someone who has a chronic illness or disability who can continue doing the things they enjoy – who is able to have a full, fulfilling life – is likely to be happier, and mentally and emotionally healthier, than someone who cannot; conversely, someone who is not sick or infirm, but is unable to do the things they enjoy – for instance, because they lack transportation, high-quality housing, or easily accessible leisure facilities – is unlikely to be able to have a full, fulfilling life, and is therefore more likely to be in poor health.
So what does that have to do with heritage? As strange as it may sound, quite a lot! This new local focus also looks back: to the interwar period and some really pioneering work done in Southwark to improve the health of local communities. To understand how radical interwar public health in Southwark was, we need to look at what living conditions were like, and how they affected public health.
Historically, many areas of the modern borough of Southwark – including Bermondsey, Rotherhithe, Walworth, Camberwell, and Peckham – had grossly overcrowded housing that was in poor condition. During the industrialisation of the Victorian era, swathes of existing housing stock was demolished to make way for factories or transport infrastructure, notably railways; if it was replaced (often it wasn’t), it was by cramming new houses into front or back gardens, or spaces that had previously been stables. Beyond that, a housing crash in the early 20th century ensured that new housing was in short supply. To raise money, both landlords and tenants divided and sub-divided what began as single-family homes, splitting them into flats, then single rooms.
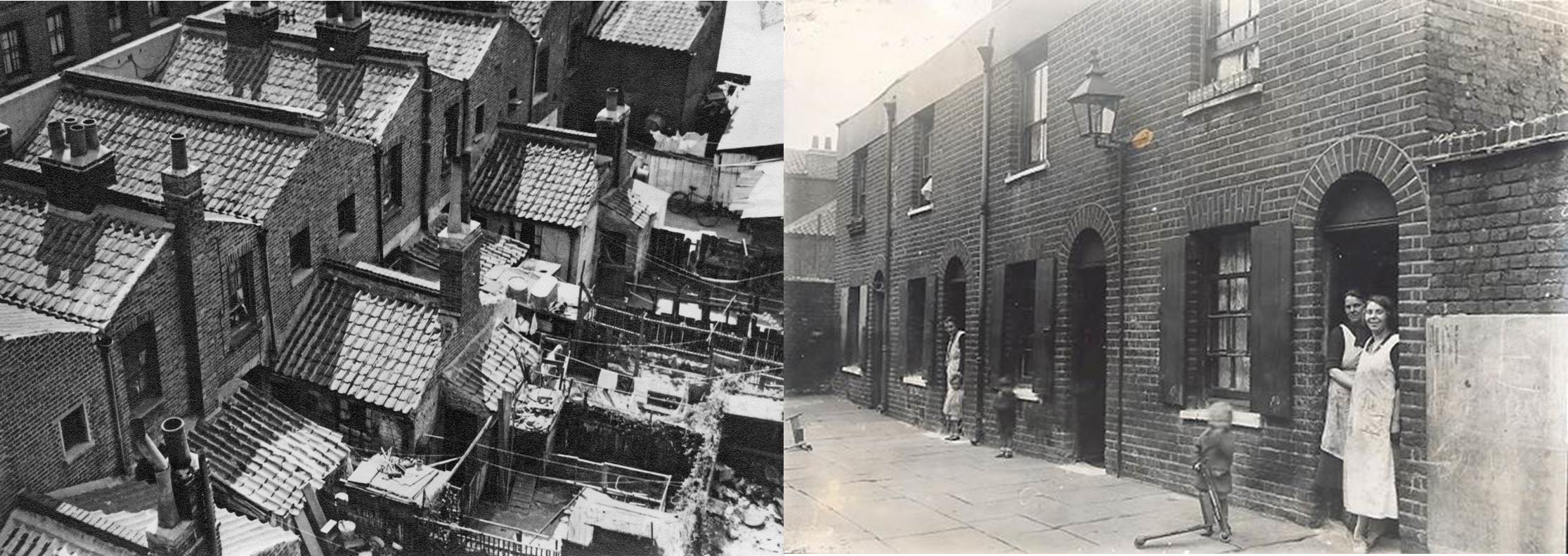
Sultan Street and Dix’s Court in the 1930s
This meant that most of what’s now Southwark was vastly more crowded than even today. In 1901, for instance, the population density of the metropolitan borough of Bermondsey was 97.62 people per acre – in 2012, the population density of London as a whole was 4 and a half times less than that, at 21.39 people per acre. In 1939, on the eve of the Second World War, 15 million Britons – fully 39% of the country’s population – lived as families in less than 1 room. In the worst cases multiple families – had one room to eat, sleep, and live in. Entire streets were filled with rows of badly-ventilated, poorly-lit “back-to-back” houses off dead-end courts, with little space for children to play, adults to get air, or even to dry laundry. There was no privacy, and little peace.
Damp and dilapidation added to the problem. The most populated areas of Southwark are close to the river, in the Thames floodplain: until the creation of the Thames Barrier in the early 1980s, storms and tides caused regular Thames floods. Houses lacked damp-proofing, and in Bermondsey – most of which was below mean high tide level – foundations were constantly wet. This meant that many houses, most of which had lathe-and-plaster interiors, had enormous damp problems.
Damp problems were made worse by the general disrepair of housing stock. At the outbreak of the First World War, three-quarters of the country lived in privately rented housing, so, just like today, rogue and negligent landlords were a problem: in some cases, a landlord might not even know they owned a property. Lack of building supplies, skilled tradesmen, and capital on landlords’ parts – an unintended side-effect of rent controls – meant that even good landlords found it hard to keep properties in good nick.
Poor quality, overcrowded housing meant poor sanitation. Most working-class housing pre-dated running metropolitan water, and so lacked specified bathrooms or indoor toilets. Subdivision of single-family houses meant the kitchen became another all-purpose living space for a family, while other living spaces lacked plumbing of any kind. Alternatively, the kitchen could be shared by the entire house. In either case, finding the time, space, heat, water, and privacy to have a bath could be all but impossible. In some flats in Bermondsey, 5 families – up to 30 people – shared a single outdoor toilet, accessible only through the kitchen on the ground floor. In all these cases, keeping house, clothes, and people clean was a vicious uphill battle – which meant the families dwelling there were constantly exposed to a variety of germs and vermin.
Southwark’s working-class families faced other hurdles to staying healthy. The first was that a high proportion of jobs involved casual manual labour – for instance on the docks. Although dockers were highly skilled, they were usually hired for short periods – a single ship, a week, or even by the day. Wages weren’t high – and more importantly, they were unreliable, making it very difficult to budget or plan spending. Because of this, families often had to eat as cheaply as possible. Eating cheaply was usually monotonous, but also lacking in balanced nutrition; then as now, fresh fruit and vegetables were often prohibitively expensive. In the interwar period, cheap food could even be dangerous: cheap milk usually came from cows who hadn’t been tested for TB. Bovines often don’t show signs that they’re ill, and can silently carry TB, shedding the bacteria in their milk. A child drinking that milk could acquire the infection, often in the bone – which could cripple or even kill.
All of the problems with housing, sanitation, and nutrition we’ve discussed created a population whose general health and immune function wasn’t very good at the best of times: to put it simply, social conditions created a population who got sicker, quicker, for longer. Even more importantly, these conditions meant that the health of individuals and communities was on a knife-edge: any sort of hard times – a father out of work for a single family, a strike for a community – could and did create serious illness and suffering.
Different areas of the modern borough were healthier than others. Specifically, Camberwell as a whole was healthier than either area to the north – probably because of its relatively well-off, relatively spacious southern end – and possibly even healthier than London as a whole. However, it’s important to recognise that even relatively healthy Camberwell had death rates that are far higher than modern British ones andthat we would now associate with the developing world. Interwar Southwark was a deeply unhealthy place, that much is clear – and people at the time knew it.

Dr Alfred Salter and his daughter, Joyce
And some pioneers decided to fight back. In Bermondsey, Alfred and Ada Brown Salter, respectively a prominent local physician and an equally prominent social worker and labour activist, lived in Storks Road – near where Bermondsey Tube station is now – with their daughter Joyce, born in 1902. Joyce was a ray of sunshine for all of Bermondsey – everyone knew her and was fond of her. But in 1910, when she was 8, Joyce caught scarlet fever for the third time. Nowadays, we call it a “Group A strep infection”, and it’s easily treated with antibiotics. But then there weren’t any – even sulfa drugs were nearly two and a half decades away. Joyce had all the love and good wishes her family and community could give: Ada and Alfred had to hang signs on their gate to update the borough, or else well-wishers would knock or ring at all hours. But that wasn’t enough, and she died in June 1910: people in Bermondsey said that their ray of sunshine was gone.
Joyce was Ada and Alfred Salter’s only child. When she died, they turned their grief into anger and their anger into action. They met with Evangeline Lowe, Ada’s best friend, and made a simple vow: the three of them would run for office at all levels of government – borough, county, and Westminster – and win. Then, together, they would do their best to, in the words of Bermondsey Labour’s 1922 manifesto, “…make Bermondsey a fit place to live in. We shall do everything we can to promote health, to lower the death rate, to save infant life, and to increase the well-being and comfort of the 120,000 people who have to live here, Bermondsey is our home and your home. We will strive to make it a worthy home for all of us”.
That meant new housing, demolishing the old, crumbling back-to-backs. New parks, like the one in St James’s churchyard, in Thurland Street, which opened in 1921: Arthur Carr, the chairman of Peek Frean’s, gave it a beautiful covered slide, the Joy Slide, that delighted local kids into the 1970s. New plants – trees planted along every verge, flowers in the parks grown in the council’s nursery in Fairby Grange, Kent, and flowers for everyone in Bermondsey with a window box to grow them in.

Ada Salter and other dignitaries pictured with the Joy Slide, 1922
Health care was another major plank in Bermondsey’s revolution. Fairby Grange was also a mother-and-baby and convalescent home: originally the Salters bought it for Alfred’s patients and conscientious objectors, but quickly donated it to the council. There was an aggressive anti-TB campaign, featuring mass X-ray screening in clinics or via a mobile service, and paid-for beds at a sanatorium in Switzerland. Bermondsey also launched an aggressive public health information campaign. Potential learning experiences were everywhere: a backlit slide-table while waiting at a clinic, leaflets into homes, even bookmarks with health slogan slipped into every book the library service issued! The public health service put floats into parades and made its own public information films. The 1925 Medical Officer of Health reports that the borough had started school exams in hygiene and home nursing – starting as early as possible to improve health.
In our next post we will look at the work of the Pioneer Health Centre in Peckham























 ‘…sleds, sliding with skeetes, a bull-baiting, horse and coach races, puppet plays and interludes, cooks, tipling and other lewd places, so that it seemed to be a bacchanalian triumph, or carnival on the water’
‘…sleds, sliding with skeetes, a bull-baiting, horse and coach races, puppet plays and interludes, cooks, tipling and other lewd places, so that it seemed to be a bacchanalian triumph, or carnival on the water’




 ots of fascinating local history. I reached out to the lovely folks here to get involved, and they have kindly welcomed me into their family as a volunteer.
ots of fascinating local history. I reached out to the lovely folks here to get involved, and they have kindly welcomed me into their family as a volunteer.













")
")


")
")
")
 1")
 One of the more significant early charities was founded by Edward Edwards and this year is the 300th anniversary of his death. In 1717 Edwards left the leases of his land and buildings to trustees, the income of which was to be used for charitable purposes. Some of the money raised was used for the construction of almshouses in the area bordered by Church Walk (now Burrell Street) and Charles Street (now Nicholson Street). The almshouses were rebuilt in 1895 with an inscription from one of the original buildings set into one a new wall. They were rebuilt once more in the 1970s and were officially opened in 1973 by Princess Anne. The new building, Edward Edwards House is now the headquarters of Southwark Charities.
One of the more significant early charities was founded by Edward Edwards and this year is the 300th anniversary of his death. In 1717 Edwards left the leases of his land and buildings to trustees, the income of which was to be used for charitable purposes. Some of the money raised was used for the construction of almshouses in the area bordered by Church Walk (now Burrell Street) and Charles Street (now Nicholson Street). The almshouses were rebuilt in 1895 with an inscription from one of the original buildings set into one a new wall. They were rebuilt once more in the 1970s and were officially opened in 1973 by Princess Anne. The new building, Edward Edwards House is now the headquarters of Southwark Charities.



